This is a guest blog post by Holly, a school-based SLP, all about speech sound disorders: articulation and phonological development.
Speech Sound Disorders
This post is a comprehensive guide to speech sound disorders, which is an umbrella term used to categorize difficulty with the production of speech sounds (the ASHA Practice Portal page for Speech Sound Disorders is a great reference for this topic).
There are speech sound disorders with known underlying causes (organic) including cleft lip/palate, orofacial conditions, deafness, dysarthria, and apraxia (check out this post for more information on childhood apraxia of speech). In this post, we’ll focus on types without a known cause (functional), including articulation and phonological disorders.
We’ll take a deep dive into these terms, but for now, here’s a quick refresher:
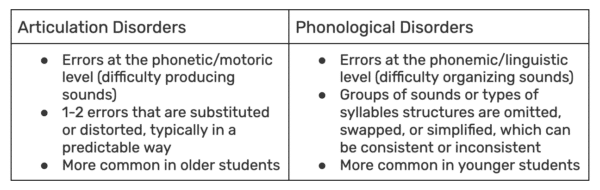
What is an articulation disorder?
An articulation disorder is characterized by difficulty producing individual speech sounds. The impairment is at the phonetic/motoric level, meaning that a sound may be substituted or distorted in a predictable way.
Example: A student produces the /s/ and /sh/ sounds with lateral airflow (e.g., a lateral lisp).
What is a phonological disorder?
A phonological disorder is difficulty organizing sounds in the brain. This impairment is at the phonemic/linguistic level, meaning that overall syllable structures and groups of sounds are omitted, substituted, or simplified. These phonological patterns often lead to reduced speech intelligibility.
Example: A student simplifies entire classes of sounds; they can produce /k/ and /g/ in isolation but habitually swaps in sounds that are produced in the front of their mouth as [t] and [d] (i.e., fronting phonological patterns, “tan” for can and “dough” for go).
Because this is a longer post, here’s an outline of everything we’ll cover:
1. Typical Speech Sound Development
– Articulation Norms
– Phonological Pattern Norms
– Speech Intelligibility Norms
– Contextual Factors
– Dialectal Considerations
3. Treatment Approaches
– Traditional Articulation Therapy
– Principles of Motor Learning
– Complexity Approach
– Phonological Contrast Approach
– Cycles Approach
– Metaphonological Approach
– Core Vocabulary Approach
– Multimodal Intervention
4. Literacy, Language, & Social-Emotional Considerations
Typical Speech Sound Development
To distinguish between typical development and speech sound disorders, let’s first consider what “typical” speech sound development looks like. We can use norms for sound acquisition, elimination of phonological patterns, intelligibility ratings, and contextual factors. For this post, we’ll also consider how dialectal differences in speech production can be distinguished from speech sound disorders. The information below is based on Mainstream American English (MAE).
Articulation Norms
There are different milestone sources to consider, which vary based on the population (who was included in the normative samples) and criteria for acquisition (what percentage of children can produce the sound at a given age, in order for it to be considered “acquired”). There is a wonderful post on the Informed SLP blog about interpreting speech norms! Here is a previous post that includes a free Speech Sound Development Chart. 🙌
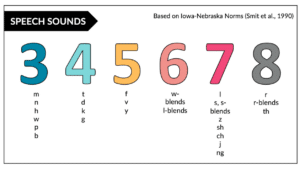
The Iowa-Nebraska norms (Smit et al., 1990) were based on monolingual children (specifically, speakers of the standard Midwestern dialect), excluding children with any known conditions such as hearing loss, repaired clefts, or motor speech impairments. This data set was used to determine at what age 90% of children have acquired a sound at the word level.
The chart below (also found in our materials collection under Therapist Tools) outlines the Iowa-Nebraska Norms for each phonetic target (articulation). When looking at each sound class (phonology), you’ll notice that young children tend to acquire nasals, glides, and stop consonants first. They subsequently go on to acquire fricatives, affricates, liquids, and consonant clusters.
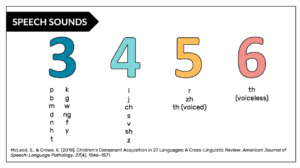
Next up, we have a summary of cross-linguistic developmental speech norms by McLeod & Crowe (2018), which included 64 studies and 27 languages. In a follow-up article (Crowe & McLeod, 2020), English consonant acquisition norms were compiled from 17 studies and a mean age of acquisition based on a criteria of 90%.
The chart below outlines the McLeod & Crowe Norms for each phonetic target (articulation). In an analysis of each sound class (phonology), plosives, nasals, and glides were typically acquired by 3;11, affricates by 4;11, liquids by 5;11, and fricatives by 6;11.
Phonological Pattern Norms
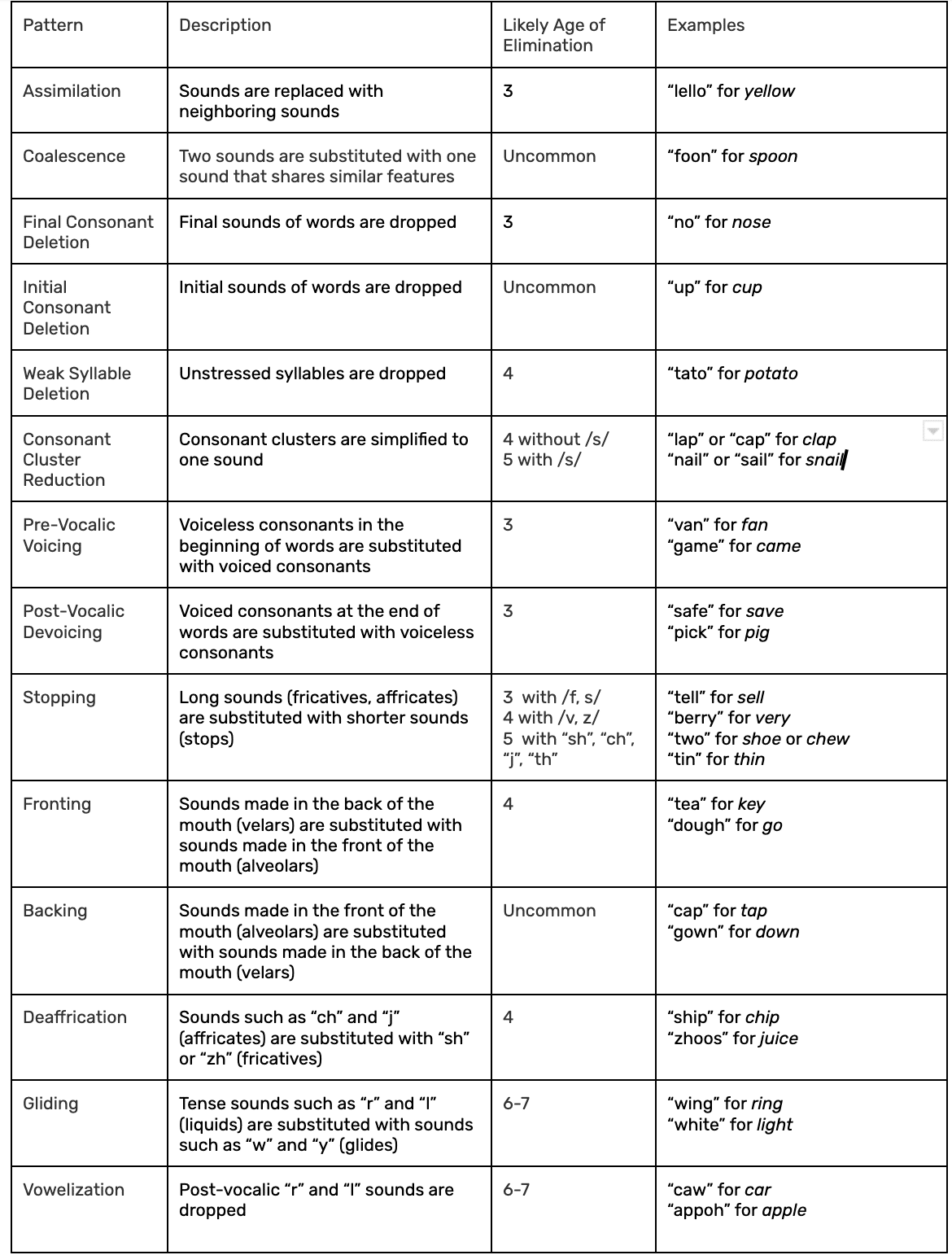
When children are learning to speak, it is natural for them to use just a few sounds and to simplify words. As their speech system develops, many of these simplified patterns are expected to fade away (phonological pattern elimination). These patterns can affect the way sounds are accidentally copied/pasted in a word (assimilation), the presence of sounds/clusters in syllables (syllable structure), and the place/manner/voicing of these sounds (substitutions).
Based on the work of Bowen (1998) and Peña-Brooks & Hegde (2015), here is a list of phonological patterns and the age that a child typically grows out of using the pattern:
Speech Intelligibility Norms
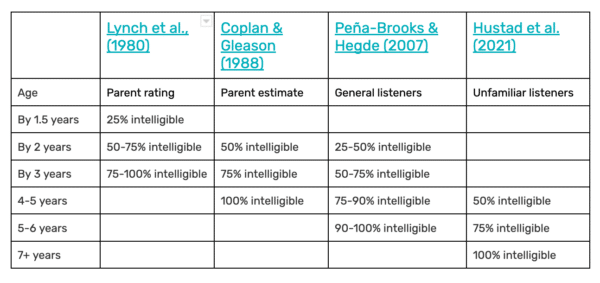
Speech intelligibility is used to determine how often a speaker is readily understood by their listeners. As you can imagine, this data may be impacted by the person judging intelligibility (a familiar listener vs. an unfamiliar listener) and the context (single words vs. utterances in connected speech; a known topic vs. a novel topic). ASHA’s guidelines state that by age 3, it’s expected that familiar people understand a child’s speech and by age 4, most people understand a child’s speech. We can also consider the following data across different sources:
To measure speech intelligibility, you can use an estimated percentage or calculate utterances using a speech-language sample. You can also gather input using a questionnaire by McLeod, Harrison, & McCormack (2012). The Intelligibility in Context Scale (ICS) has been validated across many languages and rates the degree to which a child’s speech is understood by different communication partners.
Contextual Factors
We can also consider a range of factors when determining if a student has a speech sound disorder. In an article by Storkel et al. (2019), the authors advocate for gathering student-centered information about the potential academic and social impact:
“Best practice entails using a richer representation of development, specifically reflecting the range and variability inherent in development. Moreover, diagnosing the presence of a speech sound disorder requires more than just a single measure.”
Based on these recommendations, it is valuable to consider students’ capacity for speech perception and production, overall intelligibility, stimulability, phonological awareness, academic/social impact, and student/family insights (Storkel, 2019).
The Paperwork Binder on the SLP Now Materials site has a helpful Speech Sounds Assessment Checklist that can be used to consider factors beyond standardized testing numbers (see below).
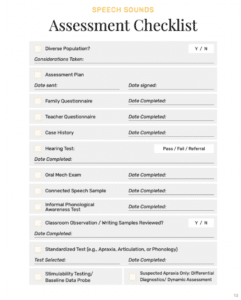
Dialectal Differences vs. Speech Sound Disorders
As clinicians, we must consider the sound systems of all the languages/dialects our students are using when we provide services. You’ll see at the top of the assessment checklist, there’s a prompt to consider factors for culturally/linguistically diverse speakers. This is important, because we don’t want to penalize students for using valid dialectal differences in their speech production.
For instance, the phonological features of African American English can include final consonant/cluster reduction at the syllable level, or substitution of “th” to /d/ and /f, t/ depending on the word position. These patterns are not counted as errors, just like a British English speaker wouldn’t need therapy to address vowelization of post-vocalic /r/. When considering a bilingual speaker, it is helpful to list out all the patterns that a student is using and cross-reference between languages to see if they could be explained by a dialectal difference or disorder. Here is a compilation of Phonemic Inventories and Cultural and Linguistic Information Across Languages from ASHA.
Differential Diagnosis of Speech Sound Disorders
Based on assessment data related to the information above, disordered speech production without a known cause can be differentiated between articulation disorders and phonological disorders. Here are some ways to distinguish between the two:
Treatment of Speech Sound Disorders
These different diagnoses lend themselves to different treatment approaches. In this section, we’ll identify which populations benefit from a variety of intervention options. Building off a previous post (Articulation Approaches), here is an expanded version:
Traditional Articulation Therapy
Who: This is appropriate for children with 1-2 errors (e.g., /s/ or /r/), who have difficulty with the physical production of certain sounds.
What: Sounds are targeted based on the order of acquisition.
When: The child’s errors are not a part of a class of sound errors.
How: Stimulable sounds are targeted first, in order of age of acquisition. Therapy activities often include auditory discrimination, shaping of target sounds, and a hierarchy of practicing in subsequent contexts (isolation, syllables, words, words, phrases, sentences, structured conversation, unstructured/carryover).
Source: Tambyraja, S. R., & Dunkle, J. T. (2014). Target Selection in Speech Therapy: Is a Non-Developmental Approach More Efficient Than a Developmental Approach? EBP Briefs, 8(5), 1-9.
Principles of Motor Learning Approach
Who: This is appropriate for children who have difficulty with the physical production of certain speech sounds.
What: Using the principles of how we learn new movements, speech sounds are taught and practiced with high levels of repetition.
When: The child has access to therapy in distributed sessions, rather than longer/massed practice.
How: We explicitly teach and shape the target sounds, then randomize practice opportunities across contexts (e.g., words, sentences, connected speech).
Source: Maas, E., Robin, D. A., Hula, S. N. A., Freedman, S. E., Wulf, G., Ballard, K. J., & Schmidt, R. A. (2008). Principles of motor learning in treatment of motor speech disorders. American Journal of Speech-Language Pathology, 17, 277-298.
Complexity Approach to Therapy
Who: This is appropriate for children with low speech intelligibility who are missing several sounds from their phonemic inventories.
What: Sounds are targeted based on the level of complexity. Research shows that children acquire skills needed for less complex sounds while working on complex sounds and that articulatory skills trickle down to foundational sounds.
When: The child doesn’t yet produce the sound and is not stimulable.
How: We target more complex, later-developing sounds first, including clusters with 2-3 sounds (like “throw” and “splash”). The objective is to make fast changes. Check out an earlier podcast episode detailing the Complexity Approach!
Source: Strokel, H. L. (2017). The Complexity Approach to Phonological Treatment: How to Select Treatment Targets. Language, Speech, and Hearing Services in Schools.
Phonological Contrast Approaches
Who: This is appropriate for children with mild-severe phonological disorders, including developmental and non-developmental errors.
What: Phonological patterns are targeted to help re-organize a child’s linguistic system by teaching meaningful contrasts between sounds and syllable structures.
When: Students consistently substitute or omit sounds using phonological patterns (e.g., fronting, backing, stopping, consonant cluster reduction, gliding).
How: We use sets of words that differ by one sound, which may deviate by one feature (minimal pairs) or many features (multiple/maximal oppositions, empty set). Using these words, students practice discriminating between the targets, then producing words in meaningful ways.
Source: Blache, S. E., Parsons, C. L., & Humphreys, J. M. (1981). A minimal-word-pair model for teaching the linguistic significant difference of distinctive feature properties. Journal of Speech and Hearing Disorders, 46, 291–296.
Cycles Approach
Who: This is appropriate for children with patterns of omissions and sound substitutions.
What: Phonological patterns are treated in cycles of 5 to 16 weeks. The error patterns are targeted in each cycle.
When: Students present with many sound omissions and some sound substitutions.
How: A new cycle begins upon completion of a previous cycle. Check out a podcast episode with Shannon Werbeckes diving into the Cycles Approach!
Source: Hassink, J. M., & Wendt, O. (2010). Remediation of Phonological Disorders in Preschool Age Children: Evidence for the Cycles Approach. EBP Briefs, 5(2), 1-7.
Metaphonological Approach
Who: This is appropriate for children with phonological disorders.
What: The phonological structure of sounds within a language is taught to help remediate the underlying lack of awareness.
When: Students lack self-monitoring skills in the area of speech sound production but are stimulable with cueing.
How: We target phonological patterns by explicitly teaching features of sounds (long/short, voiced/voiceless) and linking phonological awareness to speech production.
Source: Dean, E., Howell, J., Waters, D., & Reid, J. (1995). Metaphon: A metalinguistic approach to the treatment of phonological disorder in children. Clinical Linguistics & Phonetics, 9, 1–19.
Core Vocabulary Approach for Speech Sound Therapy
Who: This is appropriate for children with severe speech sound disorders, especially if their errors are inconsistent.
What: Select functional, high-frequency words and work on producing them consistently in a variety of contexts.
When: Students are highly unintelligible, motivated by certain interests, and where family involvement is available to support practice.
How: We collaborate with family members to create a list of target words and visuals, practicing in batches until repetition is consistent and mastery is reached.
Source: Dodd, B., Holm, A., Crosbie, S., & McIntosh, B. (2006). A core vocabulary approach for management of inconsistent speech disorder. Advances in Speech-Language Pathology, 8(3), 220-230.
Multimodal Intervention for Speech Sound Disorders
Who: This is appropriate for children with severe speech sound disorders with low speech intelligibility.
What: Supplement speech with visual supports, either using low-tech or high-tech augmentative and alternative communication (AAC) options.
When: Students and families are facing communication breakdowns and in need of a functional method of communication ASAP.
How: Simultaneously targeting natural speech and AAC speech using an integrated multimodal approach can be effective in producing positive changes in both overall communication and speech production goals.
Source: King, A., Hengst, J., DeThorne, L. (2013). Severe speech sound disorders: an integrated multimodal intervention. Language, Speech, and Hearing Services in Schools, 44(2):195-210.
Literacy, Language, & Social-Emotional Considerations
The link between speech sound disorders and additional communication concerns has been studied for good reason! Here are some resources to brush up on your knowledge in these areas:
Literacy
Not only are students with speech sound disorders at a higher risk of reading difficulties, but working on phonological awareness skills can help when targeting speech sound production in therapy (Tambyraja & McCauley, 2012). Win-win!
Because of this, phonological awareness has been a topic we’ve taken a special interest in lately on the SLP Now podcast and blog!
Blog Post: Phonological Awareness Development + Chart
Podcast #28: Where to Start with Phonological Awareness
Podcast #98: A Quick Review of Phonological Awareness
Podcast #99: Phonological Awareness Assessment and Goals
Podcast #100: Phonological Awareness Treatment Ideas
Podcast #101: What We’ve Learned About Phonological Awareness
Language
Speech sound disorders and language disorders are also known to co-occur (with rates estimated between 50-75% in preschoolers, and 15% by age 6; Macrae & Tyler, 2014). There’s still a lot of growing evidence in this area (Combiths, 2019), but something to consider is the overlap of phonological and morphosyntactic skills for students (e.g., word-final consonant clusters to mark plurals, possessives, and verb tense).
Social-Emotional Considerations
It’s no surprise that when students encounter difficulty clearly expressing themselves, the risk of social-emotional impact also rises. In a study by McCormack et al. (2009), childhood speech sound disorders were found to be associated with activity or participation restrictions related to communication, academic skills, relationships with family/friends/authority, and job skills. Because of this, it’s valuable to assess and address our students’ perceptions, feelings, and attitudes about their own speech, plus barriers they may encounter across social settings. This gives us a better picture of the impact of their speech sound disorder and leads to student-centered focus with our intervention!
—
Whew, you made it! Thanks for checking out The SLP’s Guide to Speech Sound Disorders. We reviewed typical development, considerations for differential diagnoses and intervention, plus overlapping factors with speech sound disorders! What questions do you have and is there anything else you’d like to see related to this topic?
References
Baker, E., & McLeod, S. (2011). Evidence-Based Practice for Children with Speech Sound Disorders: Part 2 Application to Clinical Practice, Language, Speech, and Hearing Services in Schools, 42(2), 140-141
Bauman-Waengler, J. A. (2012). Articulatory and phonological impairments. New York, NY: Pearson Higher Education.
Bernthal, J., Bankson, N. W., & Flipsen, P., Jr. (2013). Articulation and phonological disorders. New York, NY: Pearson Higher Education.
Blache, S. E., Parsons, C. L., & Humphreys, J. M. (1981). A minimal-word-pair model for teaching the linguistic significant difference of distinctive feature properties. Journal of Speech and Hearing Disorders, 46, 291–296.
Bowen, C. (1998). Developmental phonological disorders. A practical guide for families and teachers. Melbourne: ACER Press.
Bowen, C. (2011). Children’s speech sound disorders. Retrieved from http://www.speech-language-therapy.com/ [Updated on Tuesday, 12 October 2021]
Coplan J, Gleason JR. Unclear speech: recognition and significance of unintelligible speech in preschool children. Pediatrics. 1988 Sep;82(3 Pt 2):447-52. Erratum in: Pediatrics 1988 Dec;82(6):862. PMID: 3405680.
Combiths, P. N., Barlow, J. A., Richard, J. T., & Pruitt-Lord, S. L. (2019). Treatment targets for co-occurring speech-language impairment: A case study. Perspectives of the ASHA special interest groups, 4(2), 240-256.
Dean, E., Howell, J., Waters, D., & Reid, J. (1995). Metaphon: A metalinguistic approach to the treatment of phonological disorder in children. Clinical Linguistics & Phonetics, 9, 1–19.
Dodd, B., Holm, A., Crosbie, S., & McIntosh, B. (2006). A core vocabulary approach for management of inconsistent speech disorder. Advances in Speech Language Pathology, 8(3), 220-230.
Fabiano-Smith, L., & Hoffman, K. (2018). Diagnostic Accuracy of Traditional Measures of Phonological Ability for Bilingual Preschoolers and Kindergarteners. Language, speech, and hearing services in schools, 49(1), 121–134. https://doi.org/10.1044/2017_LSHSS-17-0043
King, A., Hengst, J., DeThorne, L. (2013). Severe speech sound disorders: an integrated multimodal intervention. Language, Speech, and Hearing Services in Schools, 44(2):195-210.
Maas, E., Robin, D. A., Hula, S. N. A., Freedman, S. E., Wulf, G., Ballard, K. J., & Schmidt, R. A. (2008). Principles of motor learning in treatment of motor speech disorders. American Journal of Speech-Language Pathology, 17, 277-298.
Macrae, T., & Tyler, A. A. (2014). Speech abilities in preschool children with speech sound disorder with and without co-occurring language impairment. Language, Speech, and Hearing Services in Schools, 45(4), 302-313.
McCormack, J., McLeod, S., McAllister, L., & Harrison, L. J. (2009). A systematic review of the association between childhood speech impairment and participation across the lifespan. International Journal of Speech-Language Pathology, 11(2), 155-170.
McLeod, S., & Baker, E., (2017). Children’s Speech: An evidence based approach to assessment and intervention. Boston: Pearson
McLeod S, Harrison LJ, McCormack J. (2012). The intelligibility in Context Scale: validity and reliability of a subjective rating measure. J Speech Lang Hear Res. 2012 Apr;55(2):648-56. doi: 10.1044/1092-4388(2011/10-0130). Epub 2012 Jan 3. PMID: 22215036.
Peña-Brooks, A., & Hegde, M. N. (2015). Assessment and treatment of speech sound disorders in children: A dual-level text. PRO-ED, an international publisher.
Shriberg, L. D., Austin, D., Lewis, B. A., McSweeny, J. L., & Wilson, D. L. (1997). The Speech Disorders Classification System (SDCS) extensions and lifespan reference data. Journal of Speech, Language, and Hearing Research, 40(4), 723-740.
Shriberg LD, Kwiatkowski J. (1982) Phonological disorders III: a procedure for assessing severity of involvement. J Speech Hear Disord. 1982;47:256–70.
Smit, A. B., Hand, L., Freilinger, J. J., Bernthal, J. E., & Bird, A. (1990). The Iowa articulation norms project and its Nebraska replication. Journal of Speech and Hearing Disorders, 55(4), 779-798.
Smit, A. B. (1993). Phonologic error distributions in the Iowa-Nebraska articulation norms project: Consonant singletons. Journal of Speech, Language, and Hearing Research, 36(3), 533-547.
Storkel, H. L. (2019) Using Developmental Norms for Speech Sounds as a Means of Determining Treatment Eligibility in Schools. Perspectives of the ASHA Special Interest Groups, Vol. 4, 67-75.
Williams, A. L. (2000). Multiple oppositions: theoretical foundations for an alternative contrastive intervention approach. American Journal of Speech-Language Pathology, 9(4), 282-288.



Leave a Reply